Tumours of the throat and larynx (Brief information)
Tumours of the throat and larynx are rare tumours among children and adolescents. They can be benign or malignant. With this text, you will receive information on these tumours, their symptoms, causes, diagnosis, treatment and prognosis.
Author: Prof. Dr. med. Dominik T. Schneider, Dr. med. Ines Brecht, Editor: Maria Yiallouros, English Translation: Dr. med. Gesche Riabowol (nee Tallen), Last modification: 2024/05/30 https://kinderkrebsinfo.de/doi/e175841
Table of contents
Tumours of the throat (pharynx) and voice box (larynx) can be either benign or malignant. However, they are rare in childhood and adolescence; in Germany, less than ten children or adolescents develop such a tumour per year.
Hence, there are no therapy studies providing the optimal treatment strategy that has been proven for many patients, as there are for other tumours in childhood and adolescence. However, the experts of the Registry for Rare Diseases in Paediatrics (German abbreviation: STEP, for "Seltene Tumorerkrankungen in der Pädiatrie") have summarized their experiences as well as the experiences of international research groups on the following pages.
Since every child is different, it is important to individually adjust the treatment to every single patient. Therefore, “STEP” offers free advice via a tumourboard attended by multidisciplinary experts. Feel free to have your attending physician contact the experts at “STEP” at step@klinikumdo.de. Also, by registering your child with the „STEP“ registry, you get the option to help expanding the experience with these rare tumours, thereby helping other children who are diagnosed with such a disease in the future.
The following paragraphs provide information on throat and laryngeal tumours that occur in childhood and adolescence.
Introduction to the throat and larynx
The tubelike throat (pharynx) connects the nose with the voice box (larynx). It also forms the connection between the oral cavity and the esophagus, thereby serving both as a food- and airway.
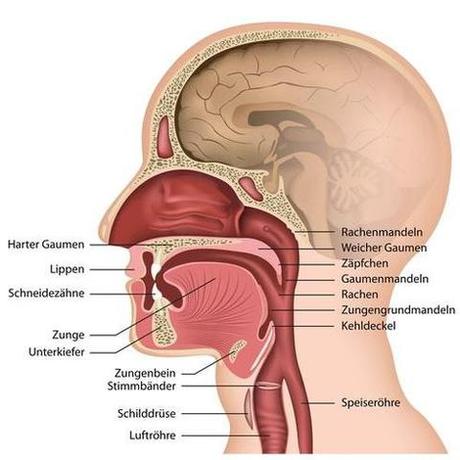
(© bilderzwerg - Fotolia.com)
The funnel-shaped voice box connects the throat with the trachea. Its upper end is firmly attached to the tongue’s hyoid, its lower end connects to the trachea. The larynx has three chores:
- It allows unhindered air passage.
- It provides for a closing mechanism that seals the airways during swallowing, so that food won’t get into the lungs.
- It is the most important organ for phonation.
Disease: what is a throat or laryngeal tumour?
Different types of benign and malignant tumours can occur in the throat and larynx; they arise from the various anatomical structures in this area (such as epithelial tissue or muscle tissue).
Squamous cell carcinomas
Very rare malignant tumours in childhood and adolescence are the squamous cell carcinomas, which arise from the squamous epithelium of the mucous membranes in the throat and larynx. For the timeframe 1968 – 2003, literature reports on 60 patients with squamous cell carcinoma in this age group, most of them between 10 and 15 years of age. Only few have been reported for preschool children. Patients with Fanconi anaemia are considered a special group (see chapter „Causes“ and „Symptoms“).
An extremely rare tumour of this region is the NUT carcinoma, which also arises from squamous epithelium. In Germany, it is diagnosed about once a year and is named after a specific gene aberration (NUT) that is found in this tumour. NUT carcinoma can develop at any site of the body (such as head and neck, chest, abdomen, each relatively close to the body’s midline), behaves very aggressively and can spread widely. Therefore, these tumours require an intensive therapy. Please seek advice in case of this diagnosis (step@klinikumdo.de).
Soft tissue tumours
Tumours of the larynx muscle (rhabdomyosarcomas) are a bit more frequent. Explicit treatment recommendations by the German Soft Tissue Sarcoma Registry (SoTiSar) are available for those soft tissue sarcomas. For information on soft tissue tumours, see here.
Germ cell tumours
Teratomas and other malignant germ cell tumours do also occur in this region. Patients with those tumours are treated according to the MAKEI protocol.
Vascular tumours
The last disease group includes vascular tumours (hemangiomas or or lymphangiomas). Classic hemangiomas in infancy respond to treatment with beta blockers (propanolol) within the first year of life. Other tumours, such as lymphangiomas, need to be removed surgically. Partially, surgery is combined with a sclerosing therapy. This treatment (also called sclerotherapy or obliteration) involves injection of a pro-inflammatory solution into the lymphangioma, which finally causes scarring, thereby making the tumor tissue shrink. Aside from this, there now are medication-based approaches that may be used successfully for some lymphangiomas. Don’t hesitate to seek advice on this.
Causes: how do throat or laryngeal tumours develop?
In contrast to children and adolescents, the most frequent cause for squamous cell carcinomas in adults is nicotin and alcohol abuse. The diseases occurring in childhood or adolescence, however, are often seen in association with human papilloma virus (HPV) infection. The infection can be transferred via the airways or from the mother to the child during childbirth. It needs to be mentioned here, though, that many children are positive for this virus without being diagnosed with a malignant tumour. Hence, additional factors (for example genetic ones), which haven’t been identified yet, may also play an important role in the development of larynx and throat cancers.
In addition, certain hereditary diseases, such as Fanconi anaemia, are associated with an increased risk to develop squamous cell carcinomas in the throat and lanrynx region. Since there is a predisposition for developing other cancers as well, Fanconi anaemia is also known as a cancer predisposition syndrome.
Symptoms: what are the signs of the disease?
The major symptoms of a larynx or throat tumour are hoarseness, cough, respiratory distress and difficulty of swallowing.
Note: because of their increased risk of tumour development (see chapter “Causes”), children and adolescents with Fanconi anaemia should, even if asymptomatic, be monitored regularly with regard to tumours of the throat and larynx with the beginning of puberty.
Diagnosis: what kinds of tests are required?
Usually, the doctor will take a detailed history (anamnesis) and perform a physical examination including a laryngoscopy and throat inspection. Laryngoscopy is done to closely assess throat and larynx; it involves a thin tube with a lens and lights being positioned in the throat after passing tongue and uvula. If laryngoscopy raises suspicion of a tumour, the next step includes assessing the tumour by endoscopy.
Imaging diagnostics such as ultrasound (sonography), magnetic resonance tomography (MRT, layered scanning of the body using magnetic fields and radio waves) and/or computed tomography (CT, detailed x-ray slices of the body) help to obtain information on the tumour’s location, its size, extent and growth pattern. When dealing with children and adolescents, not using techniques on the basis of X-rays is the goal, therefore, ultrasound and magnetic resonance tomography are the standards.
Good to know: There are no laboratory results that are specifically indicative of a throat or laryngeal tumour.
Therapy: how is treatment done?
Treatment of children and adolescents with a tumour of the throat or larynx should take place in a children’s hospital with a paediatric oncology program. Only such a childhood cancer centre provides highly experienced and qualified staff (doctors, nurses and many more), since they are specialised and focussed on the diagnostics and treatment of children and teenagers with cancer according to the most ad-vanced treatment concepts.
Complete surgical removal of the tumour is crucial as is not damaging important structures during the procedure. In case the tumour is too large for surgery or in unfavourable proximity to vital adjacent organs, an attending or preceding radiotherapy combined with chemotherapy is an option, too. Additional medications are currently being studied.
Prognosis: what are the chances of cure?
Since they are such a rarity, a statement on the prognosis of these tumours is hard to make. The chances of cure for children and adolescents with throat and larynx tumours mainly depend on the tumor type and on whether total tumour resection was doable.
Extensive squamous cell carcinomas and NUT carcinomas can be lethal despite intensive treatment. However, combined chemo- and radiotherapy can also lead to longterm survival.
Treatment can cause speech impairment. Hoarseness is quite frequent. Therefore, thorough follow-up of the patients by specialised paediatricians and ENT doctors even after completion of treatment is very important.
 PDF Brief information on throat and laryngeal tumours (176KB)
PDF Brief information on throat and laryngeal tumours (176KB)
Author: Maria Yiallouros
Status: 14/10/2023, glossary included
References 
- Hippert F, Desing L, Diez S, Witowski A, Bernbeck B, Abele M, Seitz C, Erdmann F, Brecht I, Schneider DT: Rare Tumors in Children and Adolescents - the STEP Working Group's Evolution to a Prospective Registry. Klinische Padiatrie 2022, 234: 146 [PMID: 34798669]
- Achajew A, Brecht IB, Radespiel-Tröger M, Meyer M, Metzler M, Bremensdorfer C, Spix C, Erdmann F, Schneider DT, Abele M: Rare pediatric tumors in Germany - not as rare as expected: a study based on data from the Bavarian Cancer Registry and the German Childhood Cancer Registry. European journal of pediatrics 2022, 181: 2723 [PMID: 35478271]
- Brecht IB, Bremensdorfer C, Schneider DT, Frühwald MC, Offenmüller S, Mertens R, Vorwerk P, Koscielniak E, Bielack SS, Benesch M, Hero B, Graf N, von Schweinitz D, Kaatsch P: Rare malignant pediatric tumors registered in the German Childhood Cancer Registry 2001-2010. Pediatric blood & cancer 2014, 61: 1202 [PMID: 24585499]
- Bisogno G, Ferrari A, Bien E, Brecht IB, Brennan B, Cecchetto G, Godzinski J, Orbach D, Reguerre Y, Stachowicz-Stencel T, Schneider DT: Rare Cancers in Children - The EXPeRT Initiative: A Report from the European Cooperative Study Group on Pediatric Rare Tumors. Klin Pädiatr 2012, 224: 416 [PMID: 23143769]
- Schneider DT, Brecht IB, Olson ThA, Ferrari A (Eds): Rare Tumors In Children and Adolescents. Series: Pediatric Oncology, Springer-Verlag 2012 [ISBN: 978-3-642-04196-9]
- Brecht IB, Graf N, Schweinitz D, Frühwald MC, Bielack SS, Schneider DT: Networking for children and adolescents with very rare tumors: foundation of the GPOH Pediatric Rare Tumor Group. Klinische Padiatrie 2009, 221: 181 [PMID: 19437371]